

Abstract
Introduction: Acquired thrombotic thrombocytopenic purpura (aTTP) is a rare, life-threatening thrombotic microangiopathy. A severe deficiency in ADAMTS13 activity caused by inhibitory autoantibodies leads to accumulation of ultra large von Willebrand factor (ULvWF) multimers and formation of microthrombi in small blood vessels with associated thrombocytopenia, hemolytic anemia, tissue ischemia and organ dysfunction (e.g., brain, heart, and kidneys). Caplacizumab directly blocks the interaction of the vWF A1 domain with the GPIb platelet receptor and prevents formation of microthrombi. The key efficacy and safety results of the double-blind (DB), placebo-controlled, phase 3 HERCULES study of caplacizumab for the treatment of aTTP were reported previously (Scully et al., Blood 2017 130:LBA-1). Herein, we present the results of a post-hoc analysis of the safety results normalized to time of exposure during the DB treatment period.
Methods: Patients with an acute episode of aTTP who had received one plasma exchange (PE) treatment were randomized 1:1 to placebo or 10 mg caplacizumab, in addition to daily PE and corticosteroids. A single IV dose of study drug was given before the first on-study PE and a SC dose was given daily during the PE period and 30 days thereafter. If at the end of this period there was evidence of ongoing disease, such as suppressed ADAMTS13 activity, investigators were encouraged to extend the blinded treatment for a maximum of 4 weeks together with optimization of immunosuppression. All patients entered a 28-day treatment-free follow up period after the last dose of study drug. In case of a recurrence during the DB treatment period, patients were switched to open-label (OL) caplacizumab, together with re-initiation of daily PE and immunosuppression, while maintaining the blind for the initial treatment allocation. Analysis of treatment-emergent adverse events (TEAEs) was performed on the study's safety population (i.e., all patients who received at least 1 administration of study drug). To control for differences in time of exposure, incidence rates (IR) per 100 patients months were calculated as 100 x number of events / (total number of months observed within analysis period, summed for all patients in the treatment group).
Results: The safety population consisted of 71 caplacizumab-treated and 73 placebo-treated patients. 31 patients experienced an exacerbation during the DB period, 28 in the placebo group and 3 in the caplacizumab group; 28 of them were switched to OL treatment with caplacizumab (26 of the 28 placebo-treated patients and 2 of the 3 caplacizumab-treated patients). As a consequence, the median (min; max) duration of study drug treatment during the DB treatment period, was 35 (1; 65) days for the DB caplacizumab group and 23 (2; 66) days for the DB placebo group.
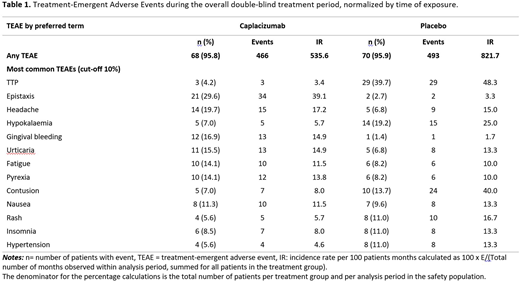
During the overall study period, at least one TEAE was reported in 69 patients (97.2%) in the caplacizumab group and 71 patients (97.3%) in the placebo group; the most frequent (occurring in >10% of patients in at least one of the treatment groups) TEAEs are presented in Table 1. After normalization for the time of exposure, the IR of any TEAE was lower in the caplacizumab group (535.6) vs. placebo group (821.7). TEAEs with a higher IR (≥5/100 patients months difference) in the caplacizumab group vs. placebo were epistaxis (39.1 vs. 3.3) and gingival bleeding (14.9 vs 1.7); TEAEs with a higher IR in the placebo group vs. caplacizumab were TTP (48.3 vs. 3.4), hypokalemia (25.0 vs 5.7), contusion (40.0 vs 8.0), rash (16.7 vs 5.7), insomnia (13.3 vs 8.0) and hypertension (13.4 vs 4.6). The IR of any SAE was 26.4 in the caplacizumab group and 83.3 in the placebo group. There were no SAEs with a higher IR (≥5/100 patients months difference) in the caplacizumab group compared to placebo. SAEs with an IR higher in the placebo group vs. caplacizumab were TTP (48.3 vs. 3.4) and anaphylactic transfusion reaction (5.0 vs. 0).
Conclusions: After normalization to time of exposure, TEAEs occuring more frequently in the caplacizumab group were epistaxis and gingival bleeding, while TTP, hypokalemia, contusion, rash, imsomnia and hypertension occurred more frequently in the placebo group. This post-hoc analysis confirms the overall good tolerability of caplacizumab for the treatment of aTTP with mucocutaneous bleeding being the most relevant risk, consistent with the mechanism of action of this drug.
Kremer Hovinga:Shire: Other: Member of Advisory Board, Research Funding; Ablynx: Other: Member of Advisory Board. Scully:Novartis: Honoraria, Other: Member of Advisory Board, Speakers Bureau. Cataland:Alexion: Research Funding; Shire: Consultancy; Ablynx: Consultancy, Other: Member of Advisory Board. Peyvandi:Ablynx: Other: Member of Advisory Board, Speakers Bureau; Ablynx: Other: Member of Advisory Board, Speakers Bureau; Novo Nordisk: Speakers Bureau; Novo Nordisk: Speakers Bureau; Roche: Speakers Bureau; Roche: Speakers Bureau; Ablynx: Other: Member of Advisory Board, Speakers Bureau; Sobi: Speakers Bureau; Sobi: Speakers Bureau; Shire: Speakers Bureau; Novo Nordisk: Speakers Bureau; Octapharma US: Honoraria; Shire: Speakers Bureau; Ablynx: Other: Member of Advisory Board, Speakers Bureau; Octapharma US: Honoraria; Novo Nordisk: Speakers Bureau; Kedrion: Consultancy; Kedrion: Consultancy; Grifols: Speakers Bureau; Octapharma US: Honoraria; Shire: Speakers Bureau; Shire: Speakers Bureau; Grifols: Speakers Bureau; Roche: Speakers Bureau; Grifols: Speakers Bureau; Novo Nordisk: Speakers Bureau; Roche: Speakers Bureau; Kedrion: Consultancy; Kedrion: Consultancy; Shire: Speakers Bureau; Kedrion: Consultancy; Grifols: Speakers Bureau; Sobi: Speakers Bureau; Octapharma US: Honoraria; Octapharma US: Honoraria; Sobi: Speakers Bureau; Sobi: Speakers Bureau; Roche: Speakers Bureau; Grifols: Speakers Bureau; Ablynx: Other: Member of Advisory Board, Speakers Bureau. Coppo:Ablynx: Consultancy. Knöbl:Ablynx: Consultancy, Other: Member of Advisory Board. De La Rubia:Ablynx: Consultancy, Other: Member of Advisory Board. Minkue:Ablynx: Employment. Sousa:Ablynx: Employment. Callewaert:Ablynx: Employment. De Winter:Ablynx: Employment. Metjian:Ablynx: Other: Member of Advisory Board.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal